Are we sharing a frustration?
I guess we are all encountering circumstances, at which we are facing difficulties to get the priority of respiratory research across. Of course, within ERS we all agree, as outlined in the European Respiratory Roadmap. But how about the rest of the world? No matter how motivated and committed we are, is the need for respiratory research sufficiently appreciated at professional levels within the government and industry? And perhaps even more importantly, at the societal level by the public and in the traditional and modern media?
I would not be surprised if this is your regular frustration when dealing with granting bodies and even when explaining your personal passion and daily job to family and friends at birthday parties… Why are colleagues in cardiovascular or diabetes research having such an easy case? And more importantly, how can we turn the tide?
Taking up the challenge
There are two ways of dealing with this. We can keep on complaining about the non-prioritised position of respiratory research whilst fighting for its position from a defensive angle. Or alternatively, just forget about this and show the professionals and public the strengths and particularly the opportunities of it. The European Respiratory Roadmap rightly provides the fundamentals of the latter strategy. But is this enough to get respiratory research concretely on the agendas of public or private research calls?
Dropping borders
There is no doubt that a new era of biomedical research is emerging. And respiratory research can take the benefit from it. The common theme of today’s success of biomedical research is ‘dropping borders’. Not only scientifically, but also strategically. If I may summarise it in a few words: the old categories of research are gone forever. For instance:
- between studies of the lung and the rest of the body (co-morbidity)
- between disease 1 and disease 2 (patient phenotypes rather than diseases)
- between cell type A and cell type B (phenotypic plasticity)
- between disciplines (integrating biology, chemistry, mathematics and medicine)
- between stakeholders (patients, care takers, scientists and policy makers)
- between steering bodies (governmental, industrial, charities)
You better be prepared, this is our play ground as of now!
Starting close by
When building the case for advocating respiratory research, I would suggest to start close by. Hence, at your regional or national level. Here, the closest interaction amongst the various stakeholders and steering bodies can be accomplished, based on more easily identified common interests. What is the recognisable burden of respiratory disease in your area (we can all use the ERS Whitebook as starting point: www.erswhitebook.org), what are the people’s most prominent needs, who are the mostly involved stakeholders, where is the outstanding quality of respiratory research, what can be the best matches here, and most importantly what are the quick wins?
The Dutch example
Sometimes small scale works. The Netherlands Respiratory Society decided two years ago to get towards: a) weighing the strengths of respiratory research in the Netherlands, b) pinpointing research opportunities, and c) prioritising areas of respiratory research. Under the charismatic leadership of Dirkje Postma the strong areas of research in the country were identified by a structured SWOT-analysis (strengths, weaknesses, opportunities, threats) based on research output and also by international peer review. This produced a matrix of strong research areas against the various respiratory diseases, together with the collectively identified, most promising opportunities.
Patients
Subsequently, this became input into a broad two-days conference, at which representatives from patients, public, care takers, researchers, government, industry, charities and policy makers were asked to set priorities during several plenary and break-out sessions. The first remarkable outcome was that there was large coherence in the choices. Hence, patients and investigators are on the same wave length when it comes to prioritising areas of respiratory research! Furthermore, patients reminded the investigators of particular opportunities and needs that surely enriched the research agenda. Finally, the concept priorities were publically discussed at a subsequent, open face-to-face meeting for anyone else interested.
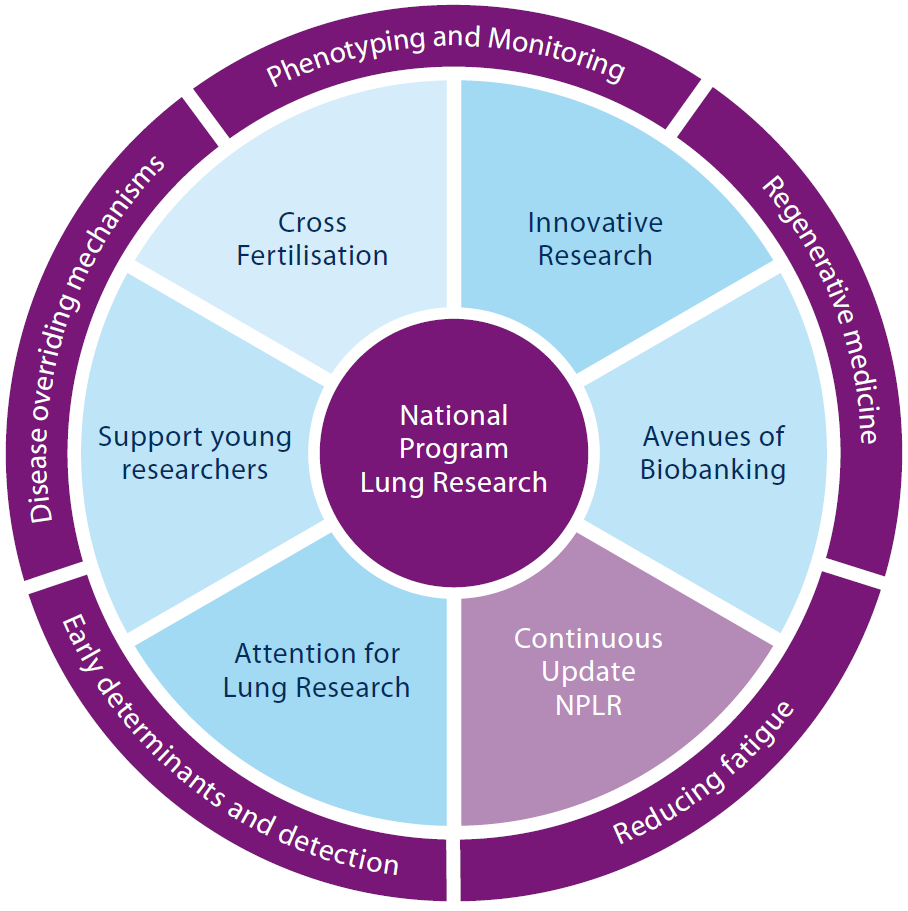
A National Programme for Lung Research
In this bottom-up way, broadly supported priorities for respiratory research were established:
- Driving mechanisms across various respiratory diseases. This includes tissue development, fibrosis, inflammation, infection, and their similarities and discrepancies across the disease spectrum.
- Phenotyping and monitoring of individual patients. This meets the demand for precision (P4) medicine, for which common databases, biobanks, protocols and eHealth procedures are needed.
- Regenerative respiratory medicine. This focuses on tissue development, -damage and -repair. This has the potential of entirely novel treatment strategies for chronic respiratory diseases.
- Reducing fatigue in respiratory diseases. Regardless of specific symptoms, fatigue is an overarching complaint of patients with respiratory diseases. Interdisciplinary biological and clinical research should take up the challenge here.
- Early determinants and detection of respiratory diseases. This aims to integrate genetic, environmental and life-style factors in the inception of disease. Early and accurate diagnostics should provide tools for primary or secondary prevention.
These 5 priorities are broad enough to host many researchers, whilst still bringing in focus. They are being fine-tuned by interdisciplinary Task Forces, including groups focusing on: Innovative Research, Cross fertilization, Young investigators, Biobanking and Advocacy.